
How would you treat this case?
July 25, 2014
This case was submitted by a team of dental faculty members in the Oral Medicine and Pathology departments of the University of Pennsylvania School of Dental Medicine.
- Alicia M. Houston, D.D.S. (Resident – Department of Oral Medicine)
- Faizan Alawi, D.D.S. (Associate Professor of Pathology – Department of Pathology)
- Eric T. Stoopler, D.M.D., FDS, RCSEd, FDS RCSEng (Associate Professor of Oral Medicine)
- Case was edited by Dr. Suham Alexander, Oasis Clinical Editor
Case Presentation

Findings
- Extraoral – NSF
- Intraoral – 2x2cm ulceration at R posterior lateral border of the tongue with indurated borders
- No herpes simplex virus found in direct fluorescent assay of lesion

Figure 1
Re-analysis of previous biopsy of the lesion reveals mucosal ulceration extending deep into the underlying regional skeletal muscle tissue (Figure 2).
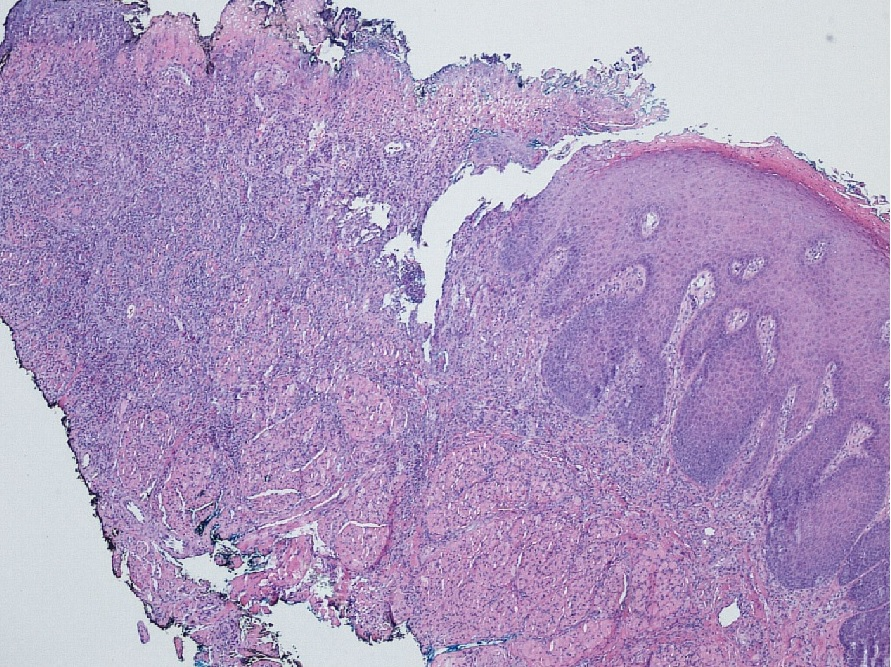
Figure 2
Histopathology reveals dense mixed inflammatory infiltrate of lymphocytes, plasma cells, large mononuclear cells include histiocytes and numerous eosinophils (Figure 3).
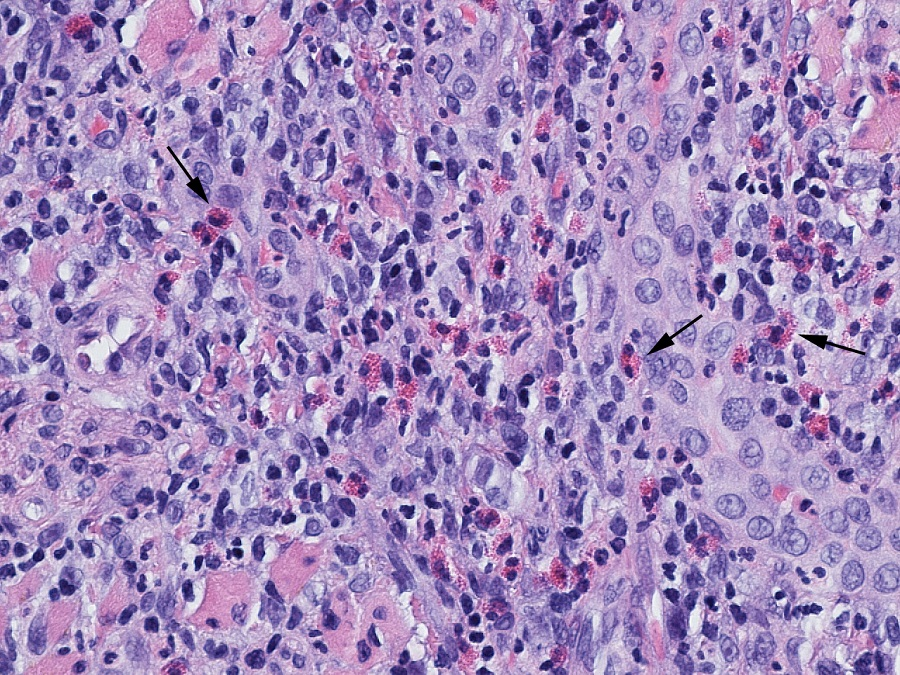
Figure 3
What is your diagnosis and treatment plan?
To view the case diagnosis and treatment, click here
The dysphasia concerns me as this irritation may be from an abnormal swallow pattern or chewing pattern. I would also smooth the teeth/restorations adjacent. Next, possibly a surgical debridement and to allow primary closure by MFS. Possibly a night guard to protect the wound during healing. The wound presents as recurrent microtrauma more than a systemic leision.
A simple therapy would be a series of Ozone gas treatment to remove the viral/bacterial load in the area to allow healing. 15 minutes with a lower tray that covers the tongue with HV suction outside the tray and a LV suction out-port opposite of the Ozone in-port. The tray can be made of siltec. Repeat every few days as needed. Supplement with Ozonated water and Ozonated oil over the area.
You may need to add a lower orthotic to increase VDO to provide the tongue more volume/space to help stop the lateral tongue thrust he/she has obviously obtained.
I would suspect traumatic ulceration aggravated by systemic health. I would focus on a combination of previous posts starting with assessing for any possible aspects intraorally that could be irritating the tongue. Sharp teeth, denture, etc. I would also assess diet/oh products for possible sensitivity reactions and seek more natural products to aid in healing. And would finish off with laser treatment to aid in healing (similar idea as the ozone, but tools I have on hand and has worked well in the past for ulcers similar to this).
Very glad to see biopsy report did not show signs of cancer, but if no healing occurs, would reassess for new biopsy in case initial biopsy missed something.
The problem with some of the previously suggested treatments is that there is no ddx. Although I would also like to have known about the condition of teeth/materials directly in the vicinity, such a lesions in my opinion should have us thinking a bit deeper. How can one submit to a treatment without any idea of what or how the problem may be arising. A blindfolded shotgun approach is really not helping anyone, and may very well disillusion the patient.
It might be worthwhile to consider systemic causes since local treatment and biopsy didn’t seem to show any significant signs of a strictly locally originating problem. The highly mixed cellularity could also be confounded/ complicated secondarily by having had a long standing open wound in the oral environment. Erosive lichen planus and major apthous ulcerations would be on my differential. Along with these it might be worthwhile to consider the problem in the context of an existing immune suppression given the history of DM, depression, polypharmacy and tendency toward contact dermatitis. To me this seems like it could very well have some immune suppression/disruption component to it. A complete blood panel with appropriate referral to the PCP and considering a multi-disciplinary approach with an oral pathologist would benefit the patient sooner rather than later.